
Rotator Cuff Repair
Specialized management by Dr. Stéphane Vasseur
Key information
- Hospitalization: 0 to 2 days
- Anesthesia: General
- Immobilization: Abduction pillow 45 days
- Dressings: Every 5 days
- Rehabilitation: 5 to 6 months
Indications
The choice of surgical treatment most often addresses young patients with important functional needs. It will be particularly favored for active people, exercising a professional activity or regular sports activities.
However, there is no age limit for surgical management, physiological age being much more important than numerical age.
In the context of trauma at the origin of the rupture, management must be carried out quickly to avoid the occurrence of intra-articular adhesions but also the risk of significant tendon retraction.
- Symptomatic tear confirmed (pain, weakness, loss of strength)
- Failure of well-conducted rehabilitation
- Active/sporting patient or high functional demands
- Favorable operability assessment (evaluation by arthro-CT/MRI)
For more information on the pathology: Rotator Cuff - Complete Pathology
Surgical treatment
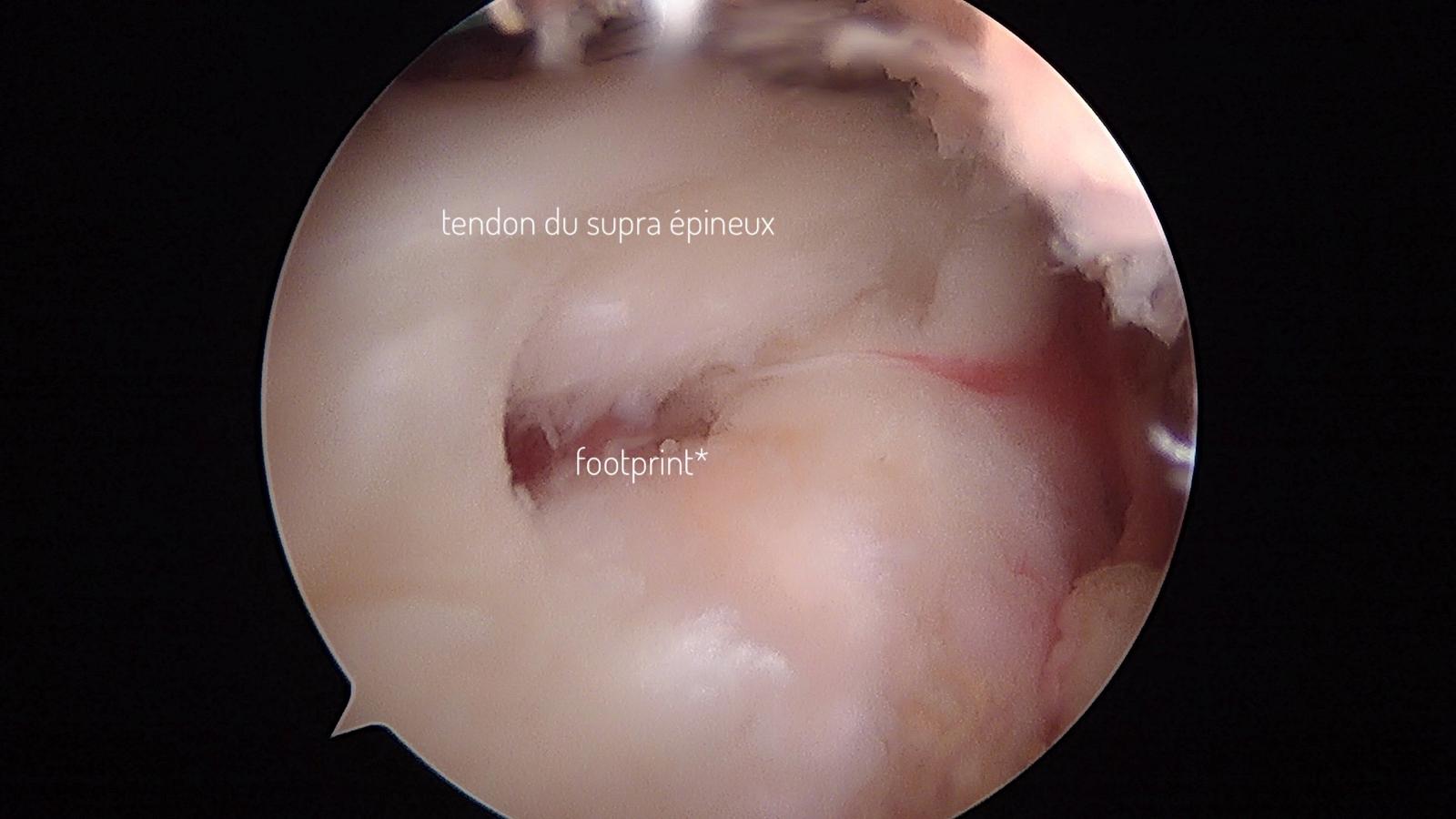
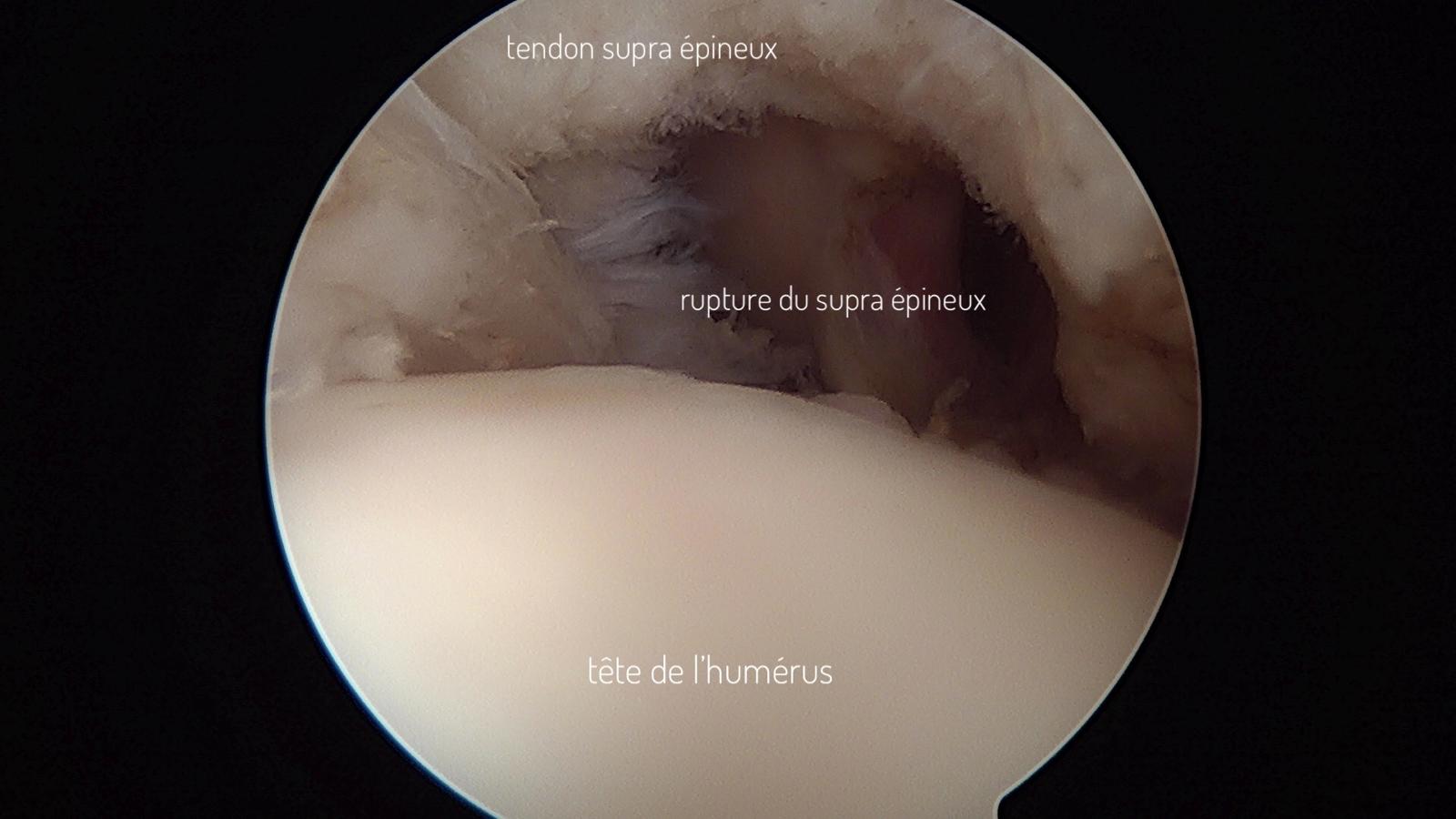
The principle of the surgical intervention is the repair/reinsertion of the torn tendon on its bony attachment at the humeral head level.
Arthroscopy
The intervention is performed under video surgery. 2 or 3 centimeter incisions in the skin allow insertion of a camera into the joint and performance of tendon repair. The absence of open surgery (large opening) limits the risks of bleeding, infection risks, muscle damage and promotes faster functional recovery.
Fixation means
Tendon repair is performed using an anchor system, inserted into the bone at the humeral head level. Suture threads mounted through the anchors allow attachment to the torn tendon and refixation at the bone level.
Double row assemblies are the reference in terms of surgical technique to obtain the best stability of the repair and maximum chances of tendon healing.
Acromioplasty
Since the anterior tip of the acromion is often at the origin of or participating in tendon lesions, the acromioplasty procedure is in the vast majority of cases performed at the same time as tendon repair.
Surgical suture with resorbable threads
Immobilization with abduction cushion
The intervention with Dr. Stéphane Vasseur takes place in the majority of cases in outpatient surgery, allowing return home the same day.
The procedure with Dr. Stéphane Vasseur takes place in the majority of cases in outpatient surgery, allowing a return home the same day.
Immobilization and rehabilitation
Immobilization of the operated arm with an abduction pillow will be necessary for a duration of 45 days. This pillow must be kept in place day and night, except for washing and during rehabilitation sessions.
Physiotherapy will begin from the first post-operative day, it will be progressive and must adapt to tendon healing.
The duration of this rehabilitation is usually 5 to 6 months, the different periods of rehabilitation must follow the physiological healing times of the tendon.
During the first 45 days
The tendon has not had time to heal and the repair only holds thanks to the sutures. It is therefore forbidden during this period to perform active movements, at the risk of causing early re-rupture of the tendon. The goal of rehabilitation in this first period is to recover joint flexibility, reduce any muscle contractures and calm post-operative pain. It is therefore essential that rehabilitation is carried out by minimizing painful phenomena as much as possible.
From day 45 to month 3
The tendon begins its physiological attachment to the bone. It is therefore possible to remove the pillow and begin active mobilization without work against resistance. It is often possible from the 2nd post-operative month to resume driving on short trips after work with the physiotherapist.
From month 3 to month 6
The tendon is healed but still fragile, it is possible to gradually resume work against resistance. Recovery of strength and endurance must never be done abruptly but on the contrary in a progressive and controlled manner to avoid the risks of recurrence and inflammatory phenomena.
Throughout rehabilitation, shoulder recentering work will be fundamental to avoid bone conflicts and painful phenomena.
Follow-up appointments with the surgeon take place at 1 month, 3 months, 6 months and 1 year post-operatively.
Risks and complications
Like any surgical procedure, rotator cuff repair can involve risks or complications. Even though the arthroscopic technique greatly reduces the risk of complications, they cannot be completely ruled out.
- Infection (rare thanks to arthroscopy)
- Bleeding/hematomas (rare)
- Tendon re-rupture or non-healing depending on tendon quality
- Stiffness, residual pain
- Nerve lesions (rare)
- Complex regional pain syndrome or inflammatory phenomena